The polycystic ovarian syndrome is endocrinopathy dominant among the women of childbearing age. This syndrome significantly affects the patient’s quality of life and by the time of menopause, it leads toward the high morbidity and mortality rate.
Polycystic ovarian syndrome is an ovarian dysfunction with hyperandrogenism, which plays a key role in worsening the condition of the patients and the morphology of the polycystic ovaries. No single diagnosis standard is adequate for the prognosis of PCOS. Clinical findings for PCOS include weight gain, hirsutism due to increased levels of androgen, irregular periods, high serum levels of luteinizing hormone (LH) and glucose intolerance due to insulin resistance. Moreover, chances of type II diabetes and cardiovascular events are doubled in patients suffering from PCOS.
Introduction
Polycystic ovary syndrome (PCOS) is the well-known endocrine disorder among females globally and it prevails with the range of 4 to 12% in females of childbearing age when they have problems in getting pregnant but PCOS can occur in any age after puberty.
It is a hormonal disorder that can cause infrequent or prolonged menstrual periods. Women with PCOS have hormonal and metabolic issues that can affect their overall health and appearance. PCOS exact cause is unknown. PCOS is common among the women of all races and ethnicities. If you are obese and your mother or sister already suffered from PCOS, your risk of PCOS may be higher.
The main culprit for the PCOS is androgen excess and leads to the development of numerous endocrine, metabolic, cardiovascular, reproductive, and psychological disorders. The excess of androgen might be due to the imbalance of hormones and insulin resistance. PCOS is a congenital disorder with sign and symptoms that appear with puberty. The major cause of the excess androgen (male hormone) levels in PCOS is unknown; however, scientists mostly associate it with family history.
Pathogenesis
PCOS is mostly related to the increased level of Anti-Mullerian Hormone (AMH) in females that affects folliculogenesis and follicles do not mature properly which affects ovulation. Moreover, raised levels of androgen hormones might be associated with reduced levels of progesterone and estrogen which ultimately cause the hypersecretion of gonadotropin-releasing hormone (GnRH) and luteinizing hormone. Therefore, the immature follicles are continuously stimulated and cause the formation of cysts in ovaries.
Signs and symptoms
Most pronounced symptoms of PCOS are acne, obesity, menstrual problems, hirsutism, infertility or subfertility, and obstetric complexities. Females with PCOS are also at high risk for glucose intolerance, type II diabetes mellitus (metabolic disorder), hypertension, dyslipidemia, vascular thrombosis and potentially cardiovascular occasions, endometrial carcinoma, ovarian cancer as well as mood swings.
Screening of polycystic ovarian syndrome
PCOS patients screening includes following:
Physical Examination
The physician should check the patient’s blood pressure, body mass index, waist size, skin discoloration, acne, and extra hair growth.
Pelvic examination
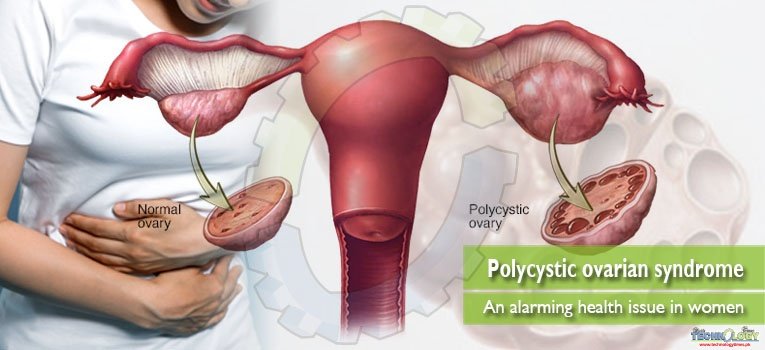
The doctor should examine the pelvic areas including vagina, cervix, uterus, fallopian tubes and ovaries for anything unusual. Pelvic ultrasonography is performed to check how the ovaries look like. The radiologist check for a cyst in ovaries and thickening of the uterus lining. Its lining may be thicker than the normal if the patient does not have periods when they are supposed to. If the patient is suffering from PCOS, the size of ovaries is usually 1 ½ to 3 times greater than the normal.
Blood testing
It is performed to measure the levels of different types of hormones such as Luteinizing hormone (LH)-a hormone that increases the ovulation but in PCOS its level is higher than normal. Follicle-stimulating hormone (FSH) and Sex hormone binding globulin (SHBG) levels are lower in PCOS patient. Estrogen is the hormone that induces periods and its level in PCOS is greater than normal. Moreover, testosterone level also increases in these patients. Anti-Mullerian hormone test shows high levels of this hormone in PCOS patients whereas this test is performed for checking the proper working of ovaries and to evaluate how far-off the menopause could be.
Diagnosis
Diagnosis of polycystic ovarian syndrome in adult females is problematic because it is considered that irregular menstrual cycle, acne, and weight gain are due to the normal hormonal changes in adolescent girls. The most common diagnostic criteria used for this age group is a high level of androgen hormone and anovulatory problems which include amenorrhea, menorrhagia, oligomenorrhea, infertility, Androgenic alopecia (hair loss) and polycystic ovaries.
Treatment
Treatment for women with PCOS may be complicated. The first step in treating these females is to schedule a session with a primary care doctor experienced in a reproductive endocrinology.
Lifestyle changes
Weight reduction in overweight women is a typical intervention. Women are recommended to reduce caloric intake and exercising to reduce at least 5 percent of their body weight. Weight reduction is most useful for those females showing symptoms of metabolic syndrome.
Medications
Treatment for Glucose intolerance
Women with PCOS need insulin-sensitizing drugs such as metformin. Metformin plays an important role in the induction of ovulation and reducing the level of glucose. These drugs also change the response of ovaries to insulin by suppressing androgen biosynthesis, theca cell proliferation, and uterine endometrial growth.
Treatment for excessive unwanted hair growth and hair loss
The remedy of excessive androgen related signs and symptoms consist of oral contraceptive pills and antiandrogens (spironolactone, flutamide, cyproterone acetate, finasteride). These medications work by blocking the effect of “male hormones (androgen)” and also by reducing the release of these hormones from ovaries. Eflornithine cream is available to slow down the unwanted facial hair growth. Laser hair removal therapies are also available.
Treatment for Irregular periods and Fertility complications
For the induction of regular periods in polycystic ovarian syndrome patients contraceptive pills or intermittent course of progestogen tablets are recommended.
Women with polycystic ovarian syndrome and infertility should be referred to a reproductive endocrinologist to discuss remedy alternatives to get pregnant. Risks related to the numerous ovulation induction medications should be discussed such as ovarian hyperstimulation and a couple of births. Clomid is the first-line ovulation induction remedy which is most commonly prescribed. The 2nd line ovulatory medicinal drug is injectable gonadotropins.
Weight loss medication and Acne treatment
Weight loss medication for overweight patients includes orlistat and statins if the patient has high levels of cholesterol in the blood. Bariatric surgical operation can be prescribed for excessively obese patients. Acne medications include topical retinoids, topical antibiotics, and azelaic acid.
Surgery
A minor surgical procedure like Laparoscopic ovarian surgery (ovarian drilling) is a surgical remedy option that could normalize the menstrual cycle and causes ovulation in females with polycystic ovarian syndrome. This system involves the use of a laser fiber or electromagnetic needle to puncture the ovary four to ten times.
Laser ovarian drilling corrects the hormonal imbalance by lowering the levels of testosterone and luteinizing hormone and increasing the levels of a follicle-stimulating hormone which helps in restoring the normal functioning of the ovaries.
Conclusion
The best management for this complex reproductive and metabolic syndrome can be originated from coordinated efforts of providers over an extensive variety of specialties. However, for the time being, we can plan to expand educational training among different specialties of the diagnostic criteria for polycystic ovarian syndrome and fundamental management methodologies with the goal that all providers are at least comfortable in generating a diagnosis and starting the treatment procedure by creating awareness among the society.
This article is jointly written by Shahrukh Samson, Wafa Majeed, Muhammad Naeem Faisal, Muqaddas Jan from Institute of Pharmacy, Physiology and Pharmacology, University of Agriculture, Faisalabad. Corresponding author can be reached at shahrukhmarium@gmail.com